Multi-Drug-Resistant Organisms and Airborne Transmission: The Overlooked Pathway
The infectious disease boardroom at a major hospital was unusually tense one morning. A cluster of unexplained infections had appeared in the bone marrow transplant unit— three cases in eight days, all involving multi-drug-resistant organisms (MDR). The usual suspects had been ruled out: no contaminated IV lines, no lapses in hand hygiene, and surfaces gleamed with fresh sanitizer. The staff were trained, vigilant, and exhausted.
“And yet,” said Dr. Sankaran (name changed), staring at the report in disbelief, “they’re still getting infected. How is this possible?”
She pointed to the chart.
MRSA. VRE. Drug-resistant Pseudomonas.
Organisms that should terrify any hospital administrator.
The question hung in the air for a long moment, until the hospital microbiologist, a quiet man in a grey coat, said softly, “What if the problem is the air itself?”
A silence followed—deep, almost uncomfortable. Airborne MDR organisms? That wasn’t part of the standard infection-control script. Not yet.
But it should have been.

The hidden journey of MDR organisms
Most people imagine airborne pathogens as tiny droplets expelled during coughing or sneezing. But MDR organisms don’t need dramatic respiratory events to take flight. They often rely on far more mundane, everyday disturbances.
A nurse changing linen.
A patient shifting on the bed.
A doctor adjusting a gown.
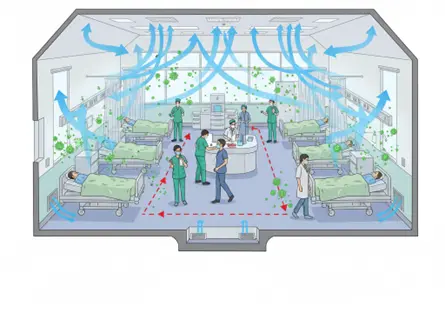
Even the gentle breeze from a swinging door.
Each of these acts sends microscopic skin flakes, dust particles, and invisible microbial hitchhikers drifting through the room. These particles can stay suspended for minutes or even hours, depending on humidity and airflow.
And MDR organisms are masters of survival.
They can cling to dust, resist desiccation, and travel on air currents generated by HVAC systems, ceiling fans, or even people walking past. The microbes may settle far from their original host—on wounds, catheters, and vulnerable patients.
This is the airborne pathway nobody wants to acknowledge, because it challenges everything we think we understand about infection control.
The data we don't like to talk about
Over the last decade, numerous studies have quietly pointed at the role of air in MDR transmission:
- MRSA has been cultured from air samples in ICUs and surgical wards.
- VRE has been found floating in transplant units.
- Carbapenem-resistant Gram-negatives have been detected in the air of high-dependency units.
- Outbreak investigations often trace contamination patterns that only airborne spread can explain.
Yet hospitals have been slow to respond because the idea disrupts traditional frameworks. Surface cleaning doesn’t solve it. Hand hygiene doesn’t solve it. PPE helps, but only partially.
To address airborne MDR organisms, you need something very different: a way to continuously remove live microorganisms from the air in real time.
This was exactly the puzzle facing Hospital X that morning.
A story of discovery
After Dr. Sankaran’s meeting, the hospital brought in an environmental monitoring team. For the first time, they sampled the air, not just surfaces. They placed microbial samplers in corners, near patient beds, by linen trolleys, and within the HVAC return ducts.
The results, when they arrived, were sobering.
Air from two rooms contained VRE colonies. Another room showed drug-resistant Pseudomonas. The HVAC return from the central corridor revealed MRSA.
“How?” asked one of the nurses, stunned.
“The air,” replied the microbiologist, “is carrying what we can’t see.”
That week, the hospital made a decision: they needed to intervene not just on surfaces, but in the airscape of the ward.
The Missing Middle: Continuous Air Decontamination
Most hospitals rely on a combination of HVAC filtration, UV in ducts, and surface disinfection. While valuable, these methods do not continuously remove live microbes from the occupied space.
This is where technologies like ZeBox create a new paradigm.
Instead of relying on passive filtration, ZeBox attracts airborne microbes and neutralizes them using an engineered microbicidal mechanism. It operates continuously, silently, and safely around patients and staff.
In other words, it focuses exactly where MDR organisms thrive:
the space between surfaces and hands—the air itself.
When Hospital X installed air-decontamination units in the transplant ward, they didn’t expect miracles. The medical director told his team, “Just treat this as an experiment.”
But within ten days, microbial air sampling showed a dramatic drop—over 80% reduction in airborne CFUs, including resistant strains. Over the next month, no new MDR infections occurred.
The staff began referring to the unit as “the invisible shield.”

What This Means for Hospitals Everywhere
If MDR organisms can move through air—and evidence strongly suggests they can—then relying solely on surface cleaning and hand hygiene is no longer enough. Healthcare settings need a three-layer defense:
- Surface decontamination
- Hand hygiene and PPE
- Continuous air decontamination
Without that third layer, MDR organisms simply remain free to drift, settle, and cause trouble.
This is especially critical in:
- Transplant units
- Oncology wards
- ICUs
- NICUs
- Dialysis centers
Post-surgical care areas
Anywhere patients have weakened defences, airborne MDR organisms can be lethal.
Rewriting the Narrative
The biggest challenge isn’t technology—it’s mindset. For decades, airborne MDR transmission has lived in the shadows of infection-control conversations.
But the experiences of hospitals like Hospital X show that acknowledging this pathway is not a sign of failure. It’s a sign of progress.
The air is the last major frontier in infection prevention, and once we begin to treat it with the seriousness it deserves, patient safety enters a new era.
A Final Scene From Hospital X
Six months later, the transplant ward is bustling again. Nurses move confidently. Patients rest peacefully. Dr. Sankaran walks through the corridor, glancing at a small, quiet device mounted near the nurses’ station.
She smiles.
“Funny,” she says to the microbiologist beside her. “We spent years fighting MDR organisms on surfaces and hands. All along, we just had to look up.”



